- 07914803818
- 02077940500 ext: 34273
- mvarcada.practice@nhs.net
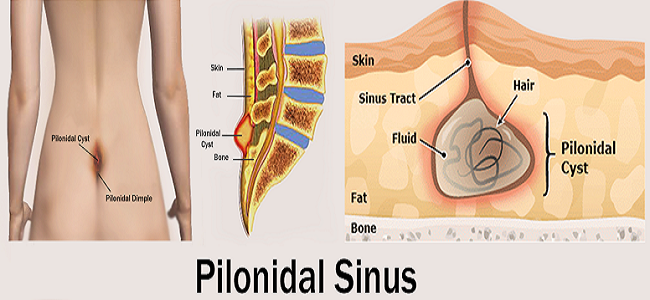
What is pilonidal sinus and who gets it?
A pilonidal sinus is a small tunnel/cavity in the skin, which is usually found at the top of the cleft between the buttocks. The cavity can become infected causing symptoms such as pain, swelling and the development of a pus-filled abscess within the sinus. If the sinus becomes infected it should be treated to prevent the infection from spreading and further complications occurring.
Who gets pilonidal sinuses?
Each year pilonidal sinuses affect around 26 in 100,000 people in the UK. It is more common in men than women and typically affects young people between puberty and the age of 40.
Risk factors and causes
Factors which increase the risk of a pilonidal sinus developing include:
What causes a pilonidal sinus?
The exact cause of pilonidal sinuses remains unclear but there are various theories used to help explain how they may occur. The underlying issue seems to be penetration of loose hairs into the skin or the blockage of a hair follicle. The area becomes inflamed and a bacterial infection is then likely to occur due to the warm and moist nature of the cleft between the buttocks.
Pressure or trauma at the affected area can cause further irritation and encourage more hair or debris to collect within the sinus. The area may become chronically inflamed/ infected with multiple sinuses joining together.
Symptoms
You may not have symptoms, although you may notice a small dimple (sometimes more than one) or depression in your skin. However, if the sinus becomes infected, you may experience symptoms such as:
Treatment
ACUTE ABSCESS
An acute pilonidal abscess is managed with an incision and drainage (I&D) procedure at the time of presentation, usually under local or general anesthesia. This management approach is consistent with simple incision and drainage of pus. Wounds are packed with gauze, and healing occurs by secondary intention in the acute setting. An I&D, however, is not the definitive procedure for pilonidal disease, as recurrence rates range from approximately 20 to 55 %.
CHRONIC OR RECURRENT DISEASE
The definitive treatment of chronic or persistent pilonidal disease is a surgical excision of all sinus tracts . The surgical procedures range from simple excision with or without primary closure to complex flap reconstruction.
Recurrence rate — Based upon research, the overall recurrence rate of pilonidal disease is 6.9 percent. Primary wound closure is associated with a significantly higher recurrence rate compared with a delayed wound closure (8.7 % versus 5.3 %)
Surgical site infections — Overall, surgical site infections (SSI) is between 8 to 10%.
Time to return to work — Patients undergoing a primary repair had a significantly faster rate of return to work compared with patients with open wounds (12 versus 18 days)